Back to Basics: Urinary Catheterization
Catheterization is the most common way to empty urine from your bladder after a spinal cord injury. Unfortunately, it is also a common source of infection.
Although you may be performing intermittent catheterization or have an indwelling catheter and using the best technique, it is important to review how and what you are doing periodically. Sometimes, it is not how you are tending to your bladder issues but your body that changes with aging. Creating a bladder program that fits naturally into your day is an important goal for individuals who need to use this method. However, ensuring that you do not become lax in the essentials is critical to your success.
Not everyone will need to catheterize. Individuals who have incomplete injuries might be able to empty their bladder on their own. Some will be able to partially release urine but still need to periodically catheterize during the day to ensure complete emptying and which is necessary to avoid bladder infections. Individuals with complete injuries will be catheterizing or have a device placed to empty their bladder.
After sustaining a spinal cord injury, your body function will be classified as upper motor neuron (UMN) injury or lower motor neuron (LMN) injury. The upper motor neuron injury tends to relate to spasticity. If you have spasticity below the level of your injury in the cervical or thoracic levels, your bladder might be spastic as well. This means that urine will enter the bladder but when a small amount is present, the bladder will spasm and an even smaller amount of urine will be expelled but the bladder will not completely empty. This leftover urine in the bladder becomes stagnant and can become more easily infected.
Lower motor neuron injury bladders are flaccid. They are associated with lumbar and sacral injuries. This type of bladder will fill with urine to overcapacity if left unattended. If you look at your legs and find them to be smaller, you probably have an LMN bladder which relates to flaccid paralysis.
 The body is quite complicated. If it was just this simple to have an upper or lower motor neuron injury bladder but it is not. Individuals can have a combination of both types of bladder function, UMN and LMN, especially if your injury is in the lower thoracic or very high lumbar areas. You could have the same level of injury as your friend, but you could have completely different types of bladder function.
The body is quite complicated. If it was just this simple to have an upper or lower motor neuron injury bladder but it is not. Individuals can have a combination of both types of bladder function, UMN and LMN, especially if your injury is in the lower thoracic or very high lumbar areas. You could have the same level of injury as your friend, but you could have completely different types of bladder function.
The three most important factors for bladder management are to:
- Empty your bladder to keep urine out of your kidneys
- Keep bacteria from entering your urinary system leading to infection
- Remain continent which will avert skin breakdown and possible embarrassment
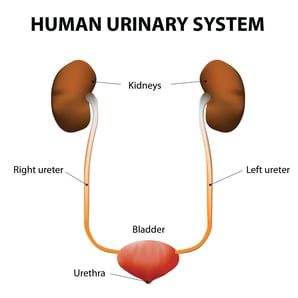
1. The bladder is a storage facility. It simply holds urine until the appropriate time and location to empty it. The kidneys process urine but do not have the capability to store urine. The ureters (there are two) are attached to each kidney. This is a one-way tube to send urine from the kidneys to the bladder for storage. If your bladder overfills and the urine does not come out of the urethra, it will back up into the ureters which will fill the kidneys. But the kidneys do not store urine so backed up urine will damage the delicate kidney tissue leading to kidney failure, damage and possible death. Yes, this is serious.
2. Urine left in the bladder will become stagnant. One little bacterium will multiply into two, two into four and etcetera. Bacteria multiply extremely quickly. Then a bladder infection is present. Concentrated urine due to dehydration is more difficult to hold and it is a better environment for bacteria to multiply. Bacteria like to collect and climb right up the ureters into the kidneys, creating a more dangerous situation of kidney infection. Therefore, drinking to keep urine a golden yellow concentration and emptying your bladder on a schedule is critical to keeping bacteria at bay. Using good hygiene and catheterization technique to keep bacteria from entering the bladder is also essential.
3. Skin is healthiest when clean and dry, not wet from bladder leakage. Urine can erode or burn the skin if left unattended leading to pressure injury. Keeping the dark, moist area of the groin is a challenge for healthy skin especially if caustic urine is present. An uncontrolled output of urine is incontinence which can be embarrassing especially when the urine is expelled in an inappropriate location.
It is important to maintain a bladder program to avoid these three costly errors. Costly in your time, quality of life and overall health. To avoid immediate issues or complications down the road, a back to basics review is a good activity to conduct.
Review your intake. This is often overlooked because people focus on the out and not the in. What goes in, must come out. Early on in your program, you might have measured your fluid intake and catheterized after taking in a certain amount of fluid. Different fluids will affect your urine output. Water is the best for drinking. Fluids with caffeine such as coffee, tea, and some energy drinks will act as a diuretic which fills the bladder more quickly. Alcohol and other sugary drinks like soda, juice and sports drinks will move through the system more quickly. Diet soda will do the same. If you drink any of these drinks, your bladder will fill more quickly.
Some people get the idea that if they do not drink much, that they will have to catheterize less. This is just not healthy for anyone. Your kidneys are working all the time. They need to keep actively processing fluid from your blood. The less you drink, the more concentrated your urine becomes which can lead to dehydration affecting the function of the kidneys as well as your bowel function, skin integrity and general health. Therefore, knowing your intake keeps your bladder, kidneys and body healthy.
There are several methods of emptying the bladder manually. Males with UMN bladders may be able to use an external catheter if their bladder will expel all the urine spontaneously. An external catheter fits over the penis. A tube carries the urine from the catheter to a collection bag. Care must be taken to ensure the elastic tape that holds the catheter does not become constrictive. Some external catheters have a sticky substance coated on the inside that will hold the catheter to the penis. These are safer than the special elastic external catheter tape but sometimes the self-stick catheters fail with an extreme force of urine.
Hygiene to the skin under the external catheter is necessary as urine is caustic. A skin prep can be used to help maintain skin. Airing of the area should occur in the morning and evening when the external catheter is changed. Also, be sure the external catheter is not creating a  pressure injury at the penile/scrotal junction. There is no successful external catheter for females.
pressure injury at the penile/scrotal junction. There is no successful external catheter for females.
Intermittent catheterization is the most often used technique to empty the bladder. In this method, a sterile catheter is inserted into the urethra at established intervals, urine is drained, and the catheter is removed. Have all supplies ready and within easy reach before starting. If your supplies or catheter touches anything except the urethra for insertion, it should not be put into your bladder. Instead, you will need another catheter or re-sterilize the catheter if that is your method.
Essential to this process is clean and thorough hand washing. Wash your hands with warm water and soap for the amount of time it takes to sing happy birthday--twice. Be extra careful around fingernails. Think of your hands as a top, side, other side and bottom. Wash up to your wrists. Rinse thoroughly and dry your hands completely.
Wash your urethra and genitalia area with warm water and soap or other cleaners. Soap can be drying to the area of the urethra so rinse thoroughly. Use a sufficient amount of lubricant to ensure a smooth catheter insertion. Drain the urine. Remove soap or cleaner so the opening to the urethra does not dry out. Dispose of supplies or clean for reuse depending on your program.
After a while, people tend to develop routines. Most will catheterize while awake about every 4-5 hours. A healthy bladder program is aimed at not catheterizing less than every four hours or waiting longer than six hours. At night, some individuals will have to catheterize due to bladder volume. Slowing (but not stopping) drinking at about 8 pm might allow you to sleep at least six hours in the night without catheterizing. Work with your healthcare professional to establish a schedule that is healthy for you.
Another helpful trick is to elevate your feet higher than your heart for an hour before your last cath of the day. This allows some dependent edema to be eliminated from your body. Always check with your healthcare professional before changing catheterization routines and timing to see if the new option will work with your personal health. Some people with medical issues will not be able to be so forgiving with the catheterization process.
Individuals with high bladder pressures, usually UMN bladder or poor hand function may have an indwelling or suprapubic catheter in place. An indwelling catheter is placed directly into the urethra. The suprapubic catheter is placed by surgically creating an opening into the bladder in the lower abdomen just above the pubic bone. A catheter is inserted into this opening.
In both cases, indwelling or suprapubic catheter, urine is continuously draining from the inserted catheter into a collection bag. A dressing is placed around the opening of the suprapubic catheter. Keep the insertion area of both catheters clean, use sterile techniques to change the catheter. Be particularly clean when changing from a day collection bag to a night bag.
Another surgical procedure for bladder catheterization is the Mitrofanoff procedure. This is typically performed in children and women but in some cases, men can take advantage of it. Access to the bladder is created surgically by making an opening from the belly button to the bladder. A catheter is then intermittently inserted into the belly button to drain urine using an intermittent catheterization schedule. The same hygiene techniques of cleanliness are used.
Pediatric Consideration: Information provided above is the same for pediatrics. Catheters will be smaller and depend on the size of your child. Catheterization is something that can be overwhelming for parents. Think of it as normal for your child. Younger children will need to be supervised when catheterizing, about fluid intake, and timing. Teens will need the same as they sometimes don’t want to be bothered with it. However, everyone toilets so they should as well. They just do it a bit differently.
Small children can learn to catheterize. When they become old enough for potty training, introduce the technique to them. They will learn at their own pace. Often children who begin school can catheterize themselves. This is a huge transition for the child and an even bigger transition for the parent. If your child is not ready at this time, you can wait a year or two, however, have a firm goal in mind. It is easy for the parent just to do the catheterization but think about your child’s independence. It is an important transition. Nurse Linda
Join Our Movement
What started as an idea has become a national movement. With your support, we can influence policy and inspire lasting change.
Become an Advocate